Contributing physicians in this story
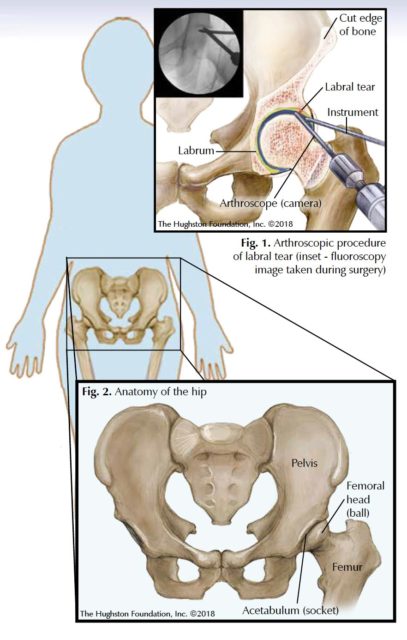 Hip arthroscopy has gained in popularity over the past 20 years due to the minimally invasive nature of the surgery and the ability to address different types of disease or injury. Surgeons primarily use arthroscopic surgery (tiny camera and instruments inserted into the joint) to remove loose bodies, which are small pieces of cartilage (tissue that covers the ends of bones) that have broken off and then move around inside the hip joint. Surgeons also use this surgery to treat labral tears, injuries to the cartilage of both the femoral head (ball) and acetabulum (socket), and femoroacetabular impingement (Fig.1).
Hip arthroscopy has gained in popularity over the past 20 years due to the minimally invasive nature of the surgery and the ability to address different types of disease or injury. Surgeons primarily use arthroscopic surgery (tiny camera and instruments inserted into the joint) to remove loose bodies, which are small pieces of cartilage (tissue that covers the ends of bones) that have broken off and then move around inside the hip joint. Surgeons also use this surgery to treat labral tears, injuries to the cartilage of both the femoral head (ball) and acetabulum (socket), and femoroacetabular impingement (Fig.1).
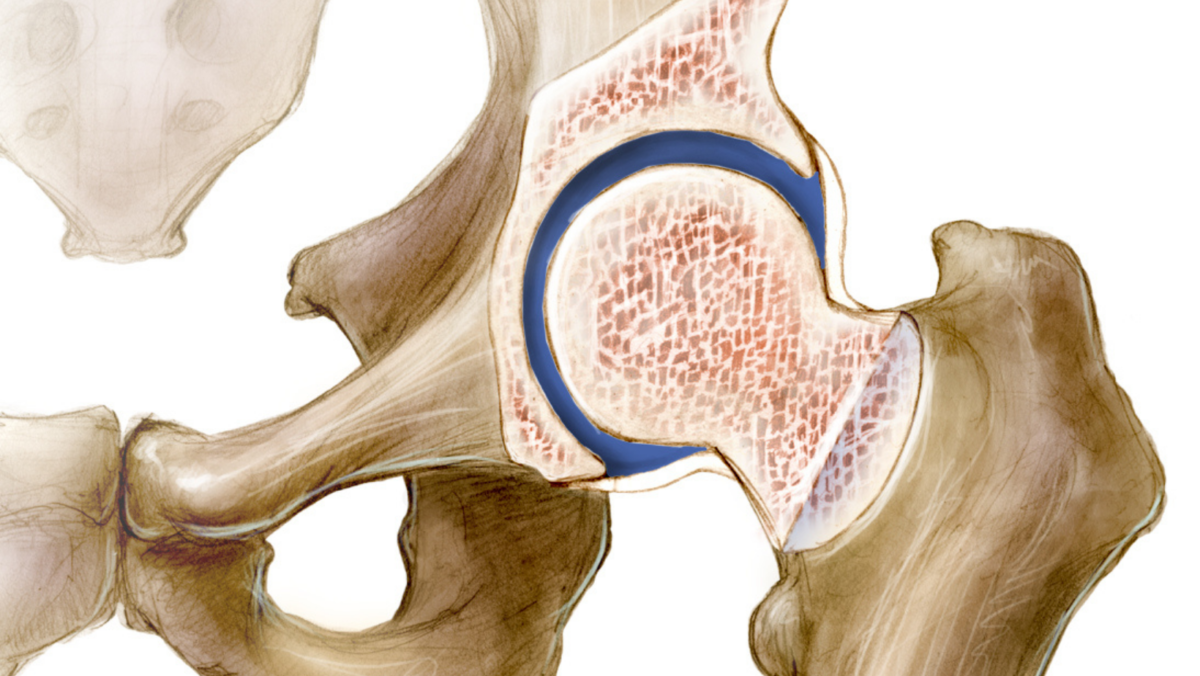
The hip joint is a ball-and-socket joint that connects the femur to the pelvis (Fig. 2). There are different elements in and around the hip joint that can be a source of pain, such as damaged cartilage and ligament (tissue connecting 2 bones) tears. When the physician evaluates a patient, it is critical to determine whether symptoms are intra-articular (coming from within the joint itself), or extra-articular (around the joint). For conditions that arise within the joint, hip arthroscopy can be a possible solution to address these problems.
Diagnosing hip pain
Your physician will complete a thorough physical exam, record your health history, and order x-rays to determine the cause of your hip pain. X-rays are a good tool for evaluating the bony structures around the hip joint. Most patients with suspected intra-articular disease who do not have obvious arthritis on x-rays will also undergo a magnetic resonance imaging (MRI) scan. A MRI is especially useful to evaluate the soft tissue structures around the hip, such as the cartilage, labrum, and tendons, which may be injured.
Nonsurgical treatment
If you have no mechanical symptoms, such as catching, popping, or a clicking sensation in your hip, your physician often begins with nonsurgical treatment. Nonoperative treatments can include resting the joint if you are involved in regular exercise or athletic activity, anti-inflammatory medications, physical therapy, and steroid injections. If these treatments fail to alleviate your pain and you continue to have difficulty either walking or standing, your physician may recommend hip arthroscopy.
Arthroscopic treatment
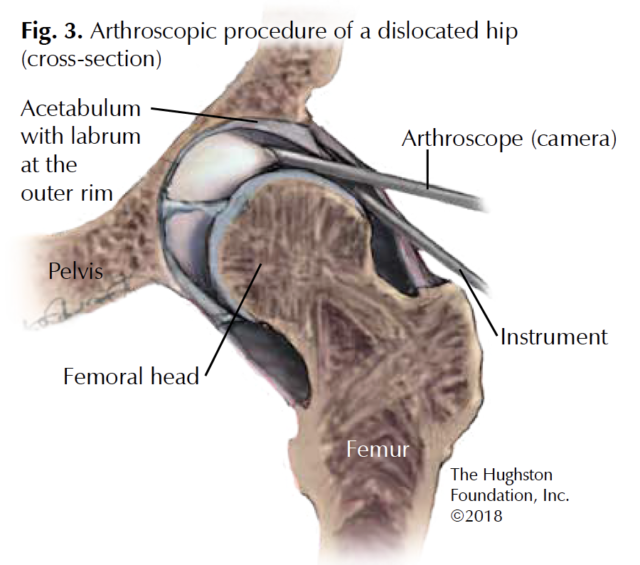
Your physician will discuss arthroscopic surgery with you if nonsurgical treatments have failed and your symptoms disrupt your normal day-to-day activities. Surgeons perform hip arthroscopy under general anesthesia and routinely use a special table to allow distraction (a gentle separation) of the ball from the socket to access to the intra-articular structures. Two common hip injuries treated arthroscopically are femoroacetabular impingement and labral tears (Fig. 3).
Femoroacetabular impingement
Femoroacetabular impingement (FAI) is a disorder of the hip in which the femoral head and neck rubs or “impinges” on the acetabulum. There are 2 types of FAI: cam impingement refers to a femoral-based disorder and is often seen in young athletic males and pincer impingement refers to an acetabular or socket-based disorder usually seen in active, middle-aged women. For both of these impingements, pain results from the proximal, or top of the femur abutting the acetabulum during range of motion, especially while bending. Patients often present with symptoms that include activity-related groin pain, difficulty sitting, and mechanical symptoms that includes a catching, clicking, or popping sensation during movement. If your physician suspects FAI, he or she will order x-rays to determine the shape and contour of the femoral head and neck as well as look for any abnormalities of the acetabulum. Your physician will also order a MRI to evaluate further the soft tissue structures in and around the hip.
At the time of arthroscopic surgery, the surgeon introduces the arthroscope into the hip joint to perform an initial diagnostic examination. Once inside the joint, the surgeon will look for disease or damage, such as cartilage defects of the femoral head and socket, loose bodies, and tears of the labrum.
Labral tears
The labrum is a horseshoe shaped structure that lines the outer rim of the hip socket. It is made of fibrocartilage and dense connective tissue. Sometimes when femoroacetabular impingement occurs, the labrum is torn. This tear can lead to pain during movement and you may experience catching, snapping, or locking. You may also feel a vague pain in your groin. If your doctor suspects a labral tear, as with FAI, you will undergo a MRI of the hip for further evaluation to confirm the diagnosis.
There are 2 main treatments of labral tears in regards to hip arthroscopy, labral debridement and labral repair. Labral tears not amenable to fixation are usually debrided, or trimmed back, to a stable base to the point that the unstable piece of torn labrum no longer causes symptoms. Your surgeon will remove any inflamed tissue in the hip joint and address any other underlying problems during surgery as well. This usually involves shaving some bone off the femoral head-neck junction as well as the hip socket so the bones do not rub against one another.
A labral repair often involves attaching the labrum back to its original site with the use of specialized anchors and sutures. Postoperatively, patients use crutches to aid in walking and are restricted to limited weightbearing and limited hip bending for approximately 4 to 6 weeks while the labrum heals.
Complications
Hip arthroscopy for either FAI or labral tears is not without complications, although the complication rate is low. Complications reported with hip arthroscopy occur at a rate between 1.3% and 6.4%. Most complications are minor and are often self-limiting, but there are several major complications that have been described in hip arthroscopy that the patient should be aware of. These include traction neurapraxia, where there is a temporary loss of motor and sensory function of nerves surrounding the hip. This occurs when traction is placed on the operative leg to help distract the hip joint in order to gain access for the arthroscope. This often resolves soon after surgery and most patients have a complete recovery. Damage to major nerves and blood vessel structures around the hip joint can also occur. Additionally, damage from instrumentation can happen; but with proper positioning and technique, the incidence of this complication is low.
On the mend
After surgery, you will be given instructions to follow for the weeks and months following surgery, including returning to see your physician for follow-up to see how you are progressing. Some of these instructions will include how to care for your portal sites and when you can shower or submerge the incisions in water. Additionally, you will be give crutches to use. Depending on the extent and type of repair, you may be on crutches for days, weeks, or months. When the hip has begun healing and the time is appropriate, your physician will refer you to rehabilitation. You should follow your rehabilitation program as instructed at the physical therapist’s office and at home. Physical therapy is a part of your treatment; therefore, you should adhere to the rehabilitation regime to achieve your best possible range of motion and functional outcome.
Hip arthroscopy can be an effective procedure and the risk of complications is low, although they do occur. Most patients are pleased with their outcomes and have resolution of symptoms, which allows them to get back to a more active lifestyle.
Author: Garland J. Gudger, Jr., MD | Columbus, Georgia
Last edited on October 18, 2021