Contributing physicians in this story
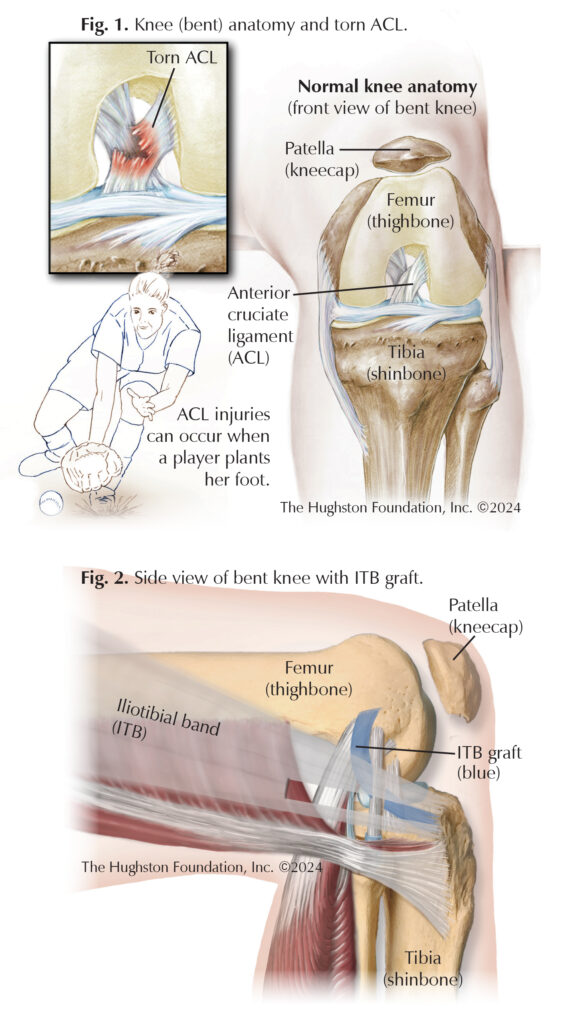
Anterior cruciate ligament (ACL) injuries commonly occur in high-performance athletes, especially during cutting and pivoting moves. The ACL is a ligament (tough connective tissue) in the knee that connects the femur (thighbone) to the tibia (shinbone). (Fig. 1). When the knee bends, the ACL provides structural support to the bones while maintaining slight elasticity, which allows dynamic, yet stable movement. With the goal of restoring ligamentous stability to the knee after an injury, ACL reconstruction is the standard treatment for safely returning athletes back to their same level of sport. Reconstruction usually involves using a tendon graft, which is a piece of healthy tendon that is transplanted surgically to replace the torn ACL. The graft is held in place with screws or other fixation devices. The tendon graft used may be an autograft (from the patient) or an allograft (from a tissue donor).
After these athletes undergo surgery, they typically require up to a year of physical therapy and rehabilitation. Despite improvements in surgical techniques and rehabilitation, ACL reconstructions can retear or “fail,” which can be devastating to the patient’s athletic career and lifestyle.
The modified Lemaire procedure, or lateral extra-articular tenodesis, has garnered recent attention due to several scientific studies showing that it can improve the stability of ACL reconstruction and even decrease failure rates.¹ The surgeon completes the modified Lemaire procedure alongside the ACL reconstruction (Fig. 2). The addition of the procedure, carries few risks and can be performed through a small 2cm incision. The surgery involves harvesting a small portion of the iliotibial band (a thick, wide tendon extending from the top of the pelvic bone to the knee joint) on the lateral (outer) side of the leg. Then the surgeon attaches the band to the lateral side of the femur to stabilize the rotational forces of the knee, thus protecting the reconstructed ACL.²
Not all patients will benefit from the Lemaire procedure. Your doctor may recommend the surgery if you play a high-risk sport that requires cutting, jumping, or pivoting, such as football, LaCrosse, soccer, or basketball. Your physician may also recommend the procedure if you have hyperlaxity (a large range of motion), high-grade rotational instability (severe instability due to ligament damage) of the knee, had an ACL injury on the other leg, or if you already had ACL revision surgery. Nonetheless, both professional and adolescent athletes can benefit from this procedure since it enhances the primary ACL reconstruction for active patients at risk for graft retears.
Author: Bradley L. Young, MD | Auburn, Alabama
References:
- Getgood AMJ, Bryant DM, Litchfield R, et al. Lateral Extra-articular Tenodesis Reduces Failure of Hamstring Tendon Autograft Anterior Cruciate Ligament Reconstruction: 2-Year Outcomes From the STABILITY Study Randomized Clinical Trial. American Journal of Sports Medicine. 2020;48(2):285-297.
- Jesani S, Getgood A. Modified Lemaire Lateral Extra-Articular Tenodesis Augmentation of Anterior Cruciate Ligament Reconstruction. JBJS Essential Surgical Technique. 2019;9(4):e41.1-7.
Last edited on December 10, 2024